Jason is now 15. He is taking AP calculus at Desert Vista High School, plays La Cross after school, is getting his driver’s permit next week, and plans to go to college and study electrical engineering after graduation. He is smart, tall for his age, and spends a little too much time playing video games.
He is also deathly afraid of peanuts.
He is afraid, in spite of the fact that he has never eaten a peanut. He has never enjoyed a Snickers bar, Reese’s Cup, or Kung Pao Chicken, and has certainly never eaten a peanut butter and jelly sandwich for lunch.
And yet, as long as he can remember, his parents have sternly warned him to stay away from peanuts. He was not allowed to eat lunch with his friend’s at school because he had to eat at a special “peanut free” table and could not have snacks brought by other parents to baseball practice because they might be “contaminated” with peanut.
His parents have had to buy three sets of Epi Pens each year to keep at school, at home, and at his grandparents home, to be used in case he had a severe allergic reaction after eating peanut by mistake. This year his family spent more than a thousand dollars on the Epi Pens.
All in all, Jason’s life and the life of his family has been complicated by the serious threat of peanut allergy. And yet, Jason is not allergic to peanut.
The problem began when Jason was just turning two. He was spending the day at his grandparent’s house and developed a rash on his cheeks and vomited. His parents became concerned that he may have had an allergic reaction to something he ate and so took him to his pediatrician who decided to run a food allergy panel just to be sure.
The test came back positive for peanut. The pediatrician suggested that it might be best for Jason to avoid peanuts since if was unclear if he may have eaten something that contained peanut at his grandparent’s house. His parents read a story about a child with severe peanut allergy who died after being kissed by someone who had eaten a peanut and so requested an Epi Pen to keep on hand. All family members, friends, and teachers, were instructed on the importance of strict peanut avoidance when around Jason and on the use of an Epi Pen.
I saw Jason for first time six months ago. His parents needed a refill of the Epic Pens and since his pediatrician was no longer practicing, they decided to make an appointment with an allergist.
After talking with Jason and his mother, it was clear that Jason did have allergies. He sneezed frequently, complained of stuffy nose and itchy eyes during the spring and fall, particularly while playing La Cross, and on occasion had wheezing and chest tightness after spending time around a friend’s cat. Mom was not concerned about these symptoms, lot’s of people had them, but she with very concerned about his severe peanut allergy.
Because of his history, allergy testing to pollen, cat dander, and peanut was completed. The results showed very strong reactivity to grass, tree, and weed pollen as well as to cat dander. The skin test to peanut was also mildly positive.
How do we interpret these results? Most importantly, is Jason allergic to peanut?
To begin we rely on three sources of information to help us make a diagnosis of allergy: the patient’s history, laboratory tests, and a food challenge.
In Jason’s case, the history is not very strong for peanut allergy. In fact, it is not clear if he has ever been exposed to peanut.
What about the positive blood test and skin test for peanut allergy?
Both tests rely on the detection of a specific antibody produced by the body that reacts with peanut. When we find these antibodies, called IgE or immunoglobulin E, we can say that the patient shows sensitization to the food being tested. Both the blood test run when Jason was two and the recent skin test are technically not allergy tests, but tests for sensitization.
This distinction in terminology is important because many people have sensitization to a food (based on skin or blood tests) that they have eaten their entire lives without problems. Since food allergy by definition is adverse symptoms caused by exposure to a food that a patient is sensitized to, then without symptoms, there is no allergy.
If we define a perfect food allergy test as being reactive or positive in 100% of patients who have true allergy to the food and non-reactive or negative in 100% of patients who are tolerant of the food, meaning it is safe for them to eat it, then conventional food allergy testing is not very good. In fact, conventional food allergy testing has an approximately 50% false positive rate: Half of the patents that test positive to a food on these allergy tests are NOT allergic to the food. The test’s ability to rule out allergy is better, by some estimates more than 90%: There is less than a 10% chance that a patient with a negative test to a food will have an allergic reaction if they eat the food.
When we say that conventional allergy tests for peanut allergy have a 50% false positive rate we do not mean the test result is an error or mistake. The test accurately detects allergic or IgE antibodies to peanut. But as was mentioned, the presence of these antibodies does not always cause problems when the patient eats peanut and therefore is considered a falsely positive test for food allergy.
To understanding WHY we can have allergic antibodies to a food that we tolerate it is helpful to understand a few things about proteins. You can find a brief introduction to proteins here.
Peanuts, as well as most other foods, contain multiple proteins. The proteins in peanut are given numbered names beginning with Ara h (from the scientific name for peanut Arachis hypogaea). The peanut proteins Ara h1, Ara h2, Ara h3, Ara h6, Ara h8, and Ara h9 have been detected and allergic IgE antibodies have been found that react with each of these proteins.
Some of these peanut proteins, such as Ara h8, are very similar to proteins found in pollen produced by allergenic plants. In fact, if a patient is allergic to birch tree pollen, the anti-birch tree IgE antibodies they produce are likely to react with the Ara h8 protein in peanut. Patients with allergic antibodies to Ara h8 alone rarely have significant peanut allergy and yet will have a positive skin or blood test to peanut. One study showed that 79% of patients who had allergies to pollen reacted positively to peanut on an allergy test but were tolerant of peanut.
Other studies have shown that patients with high levels of allergic antibodies to the Ara h2 protein in peanut are more likely to have true peanut allergy. These observations have led to the development of component allergy tests were a patients blood can be tested for allergic antibodies to a specific food protein, not just the whole food.
Component testing for peanut allergy does show improved diagnostic accuracy compared with conventional blood tests, although it continues to have a high false positive rate and unfortunately can also be negative in patients who have true peanut allergy.
Component allergy testing for peanut was ordered for Jason and the results showed positive to Ara h8 only suggesting that the positive result on the skin test and earlier blood test occurred because of his strong sensitivity to pollen.
The results were discussed with Jason’s parents who asked if there was any other test that might be used to confirm that he is not allergic to peanut.
In fact, the most reliable and considered to be the gold standard for making a diagnosis of food allergy, is the double-blind, placebo-controlled food challenge. In this test, the patient is given a sample of the test food as well as a sample of a similar, non-allergic food as a placebo. Double blinded means that the doctor and technicians conducting the challenge as well as the patient, do not know which is the real test food and which is the placebo. The test is considered positive if the patient shows obvious signs of a reaction after eating the test food but not after eating the placebo.
There are a number of problems with the double-blind, placebo-controlled food challenge: It is difficult to perform, requiring significant time and recourses; A patient can have a severe allergic reaction to the food and therefore the study must conducted by trained personal in a setting that is capable of handling a severe emergency; and it is not always possible to find a suitable food to serve as a placebo.
Because a food challenge carries the very real risk of a severe allergic reaction it is rarely done if either the history or laboratory tests strongly suggest allergy. Open challenges to a food conducted in the allergist office is considered to be an alternative to a blinded, placebo-controlled challenger if the likelihood of significant allergy is considered to be very low based on history and previous tests.
Because of the weak history for peanut allergy and the results of component allergy testing, a peanut challenge in the office was offered to Jason and his parents.
When the food challenge was discussed with Jason he became very anxious and said that he did not see any reason to do it since he has done well staying away from peanut his whole life. He said he felt sick just thinking about it.
Hopefully, Jason’s fear of peanut allergy will subside with time and education and he will someday be able to enjoy a peanut butter and jelly sandwich or Snickers Bar. And hopefully, improved testing methods as well as better understanding of food allergy will make such cases of unnecessary fear and anxiety over something to be enjoyed a thing of the past.
Brian Millhollon, MD




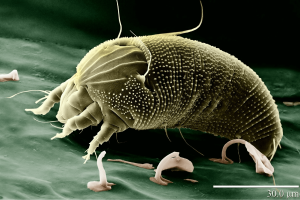
 Innumerable numbers of these microscopic insects eat, grow, raise families, and poop in the part of the home were we spend most of our time, the bedroom. They like our beds because it provides a rich source of their favorite food: people dander. House Dust Mites feed on the dead skin scales (dander) than we leave behind while tossing and turning trying to get our 8-10 hours. After a zillion generations of living, eating, pooping, and dying in our beds, the accumulation of house dust mite related “material” in our mattresses, pillows, and comfy down comforters can be disgustingly rich. And all of this is allergenic.
Innumerable numbers of these microscopic insects eat, grow, raise families, and poop in the part of the home were we spend most of our time, the bedroom. They like our beds because it provides a rich source of their favorite food: people dander. House Dust Mites feed on the dead skin scales (dander) than we leave behind while tossing and turning trying to get our 8-10 hours. After a zillion generations of living, eating, pooping, and dying in our beds, the accumulation of house dust mite related “material” in our mattresses, pillows, and comfy down comforters can be disgustingly rich. And all of this is allergenic.
 This is a picture of the hydrometer’s current reading. The indoor humidity has stayed around 30-40% during our most humid time of year with a rare spike to just above 50% during a recent storm. These humidity levels are too low to support House Dust Mite growth.
This is a picture of the hydrometer’s current reading. The indoor humidity has stayed around 30-40% during our most humid time of year with a rare spike to just above 50% during a recent storm. These humidity levels are too low to support House Dust Mite growth.






 I took up cycling 5 years ago (mid-life crisis or early onset dementia?) and like most of the local lycra-ed community trying their best to out-pedal old age, Pecos Road became my second home; the place for serious training when long intervals were needed or to join friends for group rides and the occasional kamikaze sprint at the roads end. On Pecos you could spread you wings and fly for miles.
I took up cycling 5 years ago (mid-life crisis or early onset dementia?) and like most of the local lycra-ed community trying their best to out-pedal old age, Pecos Road became my second home; the place for serious training when long intervals were needed or to join friends for group rides and the occasional kamikaze sprint at the roads end. On Pecos you could spread you wings and fly for miles.